
Pulmonary Embolisms - What are they?
- Brandon Schoborg
- Apr 27, 2022
- 3 min read
It's been a while since we've left you with a blog post, so hopefully this one was worth the wait. In this post, we are going to cover pulmonary embolisms. Through our initial education programs, I feel like we've had this elusive and deadly "phenomenon" drilled into our heads from a signs and symptoms perspective along with the "diesel bolus," but we often don't dive too deep into them as a whole.
In this post, we hope to do the following:
•Review the physiological effects of the pulmonary embolism.
•Understand where most pulmonary emboli originate and why.
•Discuss the “stereotypical” increased risk factors associated with pulmonary emboli.
•Discuss the correlation between pulmonary embolisms and the transgender community.
THE STATS

237,000 non-fatal pulmonary embolisms occur in the US each year
294,000 fatal pulmonary embolisms occur in the US each year
These numbers should jump off the page and grab you...as it's not often that we encounter something that kills more patients than it spares.
THE PATHOPHYSIOLOGY
Obstruction of the pulmonary artery or one of its branches by a thrombus that originates somewhere in the venous system or in the right side of the heart. Most commonly, a pulmonary embolism (PE) begins as a deep vein thrombosis (DVT) = thrombus formation in the deep veins, typically the calf or thigh, but can occur in the arm.
This leads to a V:Q mismatch (ventilation:perfusion). Arterial hypoxemia is compensated by "blowing off" more CO2 than is necessary (increasing the respiratory rate).
TYPES OF CLOTS

VIRCHOW'S TRIAD - DVT PREDISPOSITION
Discovered by Dr. Rudolf Virchow

Intravascular Vessel Damage:
•Damage alters the dynamics of blood flow
•Can result from smoking, chronic HTN, atherosclerosis
•When damage occurs, “turbulence” occurs
Turbulent flow:
Occurs when rate of blood flow becomes too rapid; creates a disordered flow or “eddy currents” = increasing the friction within the vessel.
Can be caused by plaque formation, vessel bifurcations, stenosis or vascular disease.
Stasis of Flow
•More likely to occur in patients with A-Fib, valvular heart disease or prolonged immobility.
•Decreased/slow blood flow causes an interaction with surface proteins that lead to thrombi production.
Hypercoagulability
•Can occur in the presence of a variety of conditions:

•Pregnancy
•Oral contraceptive medications
•Cancer (lung & pancreatic)
•Chemotherapy medications
•Inherited thrombophilias
PULMONARY EMBOLI & PREGNANCY
During Pregnancy
Uterus compresses against the iliac vein - not allowing blood to return, therefore clots develop. When this clot becomes dislodged and travels to the lungs, it is named a "pulmonary embolism."

After Birth
Amniotic fluid/micro clots leak into the lacerations in the uterus, enter the blood stream and eventually become lodged in the pulmonary system. When this occurs, it is named "amniotic fluid embolism."
ORAL CONTRACEPTIVES AND BLOOD CLOTS
•17% of females of childbearing age take some form of oral contraceptive
•Increased estrogen and progesterone levels lead to increased clotting mechanisms
•Increases triglyceride levels
•Increases RBC concentration
•Lowers good cholesterol & increases bad cholesterol

THE TRANSGENDER COMMUNITY
•Per the American Heart Association (AHA, 2019), Male sex at birth transitioning to female had an elevated risk of cardiovascular disease
•Analysis of 2,500 transitioning women
•2X as many strokes
•2x the amount of MIs
•5x the amount of DVTs

CLINICAL PRESENTATION
Patient's experiencing a pulmonary embolism will generally have a sudden onset of dyspnea, chest pain, tachypnea, tachycardia, hypocapnia and hypoxia. When encountering a patient with an acute onset of any of the above symptoms and no significant past history that correlates, definitely keep PE at the forefront of your differential diagnoses.
If left untreated long enough, a pulmonary embolism will eventually result in obstructive shock. The pulmonary artery blockage causes a tremendous strain on the right ventricle which leads to right ventricular hypertrophy and right ventricular strain. Ultimately, a significant reduction in preload and cardiac output occur.
IN-HOSPITAL TESTING & TREATMENT
Lab Values & Testing

Well's Criteria (see image)
CBC, ABG, BMP, D-Dimer
Contrast Pulmonary Angiogram (CTPA)
V/Q Scan
Chest X-Ray (CXR)
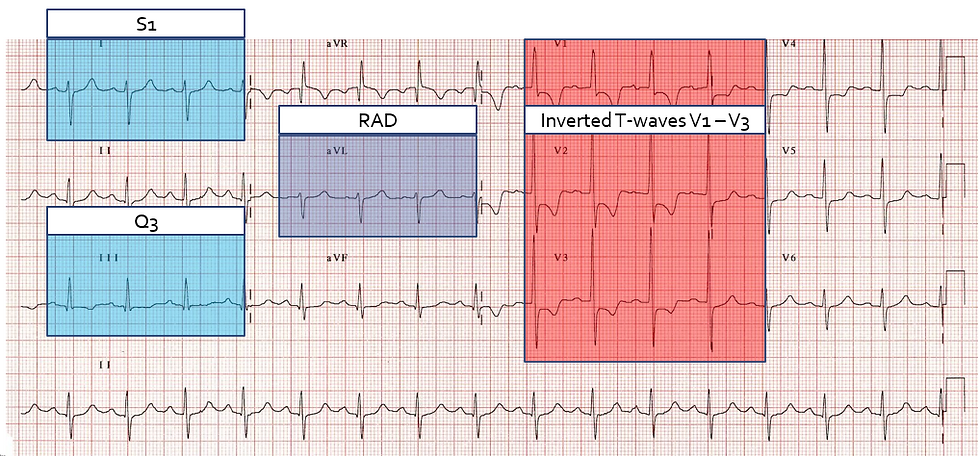
12 Lead ECG
Treatment

Sources
https://www.ems1.com/ems-products/capnography/articles/4-things-ems-providers-need-to-know-about-pulmonary-embolism-4I1Wv13PRksPyI0I/#:~:text=Because%20pulmonary%20embolism%20obstructs%20pulmonary,sounds%20strongly%20suggest%20pulmonary%20embolism.
https://williamsinstitute.law.ucla.edu/wp-content/uploads/Trans-Adults-US-Aug-2016.pdf
https://www.ncbi.nlm.nih.gov/books/NBK539697/
-Pass with PASS, LLC
Comentários